




Professional Association Membership
Examine the importance of professional associations in nursing. Choose a professional nursing organization that relates to your specialty area, or a specialty area in which you are interested. In a 750-1,000 word paper, provide a detailed overview the organization and its advantages for members. Include the following:
- Describe the organization and its significance to nurses in the specialty area. Include its purpose, mission, and vision. Describe the overall benefits, or “perks,” of being a member.
- Explain why it is important for a nurse in this specialty field to network. Discuss how this organization creates networking opportunities for nurses.
- Discuss how the organization keeps its members informed of health care changes and changes to practice that affect the specialty area.
- Discuss opportunities for continuing education and professional development.
Prepare this assignment according to the guidelines found in the APA Style Guide, located in the Student Success Center. An abstract is not required.
This assignment uses a rubric. Please review the rubric prior to beginning the assignment to become familiar with the expectations for successful completion.
References:
Explore the Advocacy page of the American Nurses Association (ANA) website.
URL:https://www.nursingworld.org/practice-policy/advocacy/
Read Chapter 5 in Dynamics in Nursing: Art and Science of Professional Practice.
this is the chapter 5
By June Helbig
nurses provide services that maintain respect for human dignity and embrace the uniqueness of each patient and the nature of his or her health problems, without restriction with regard to social or economic status. (American Nurses Association, n.d.a, para 1)
Essential Questions
- What significance does joining a professional organization have on nursing practice?
- How can nurses contribute to legislative changes that impact nursing practice and patient outcomes?
- Why is evidence-based practice (EBP) the gold standard in patient care protocol improvements?
Introduction
According to the American Nurses Association (ANA) there are currently 3.6 million registered nurses in the United States (American Nurses Association [ANA], n.d.b, para 12). The ANA is a professional nursing organization, which began when fewer than 20 nurses attended a convention in 1896. Nurses at the time were concerned with nursing practice standards and nurse competency. The ANA has since grown into an organization with interests in improving health care and setting standards for nursing practice. All nurses are represented regardless of status within the organization. The goal of professional organizations is to support nurses and improve the profession (ANA, n.d.c).
This chapter will explore the significance of joining professional organizations and how nursing can contribute to legislative changes that may affect patient outcomes as well as the work environment of the nurse. Professional nursing organizations are responsible for the development and certification of nurses interested in improving health care and providing safe quality nursing care. Through participation in professional organizations, nurses can actively contribute to legislative changes that can affect patient care and the way they conduct their work. Nurses are continually looking for and exploring new ways to provide patients with quality care. Nurses perform studies looking for new and innovative ways to provide care. The use of evidence-based practices (EBP)has become the gold standard for providing safe, quality care to patients.
Standards applied to nursing care include:
- ANAs Standards of Practice
- The Joint Commissions National Patient Safety Goals (NPSGs)
- Structured communication tools
- Integrated health care priorities
- Quality and Safety Education for Nurses (QSEN)
- Social determinants of health
- Cultural competence
- Healthcare and Research Quality Act of 1999
Standards of Nursing Practice
Standards of practice are rules and regulations that guide the nursing practice. The Nurse Practice Actis a law in each state regulating nursing practice. The National Council of State Boards of Nursing (NCSBN), founded in 1978, requires the licensed registered nurse (RN) to have specialized knowledge, skill, and independence in decision making. Originally, the NCSBN was part of the American Nurses Association Council of the State Boards of Nursing. The NCSBN was created to protect the public from incompetent or unlicensed health care personnel. The NCSBN has the responsibility of providing regulatory excellence for public health, safety and welfare, and protecting the public by ensuring that safe and competent nursing care is provided by licensed nurses (National Council for State Boards of Nursing [NCSBN], n.d.a, para. 1).
Information about licensure is available from each states board of nursing as well as from Nursys. Nursys is the only national database for verification of nurse licensure, discipline and practice privileges for RNs and LPN/VNs licensed in participating boards of nursing, including all states in the Nurse Licensure Compact (Nursys.com, n.d., para 1).
ANAs Standards of Practice
In addition to the rules and regulations that govern nursing practice, the ANA wrote the Standards of Practice, which are used along with the state Nurse Practice Act to guide safe practice. It is important for the RN with a Bachelor of Science in Nursing (BSN) degree to be aware of the rules and regulations that govern nursing. The standards of practice describe a competent level of nursing practice demonstrated by the critical-thinking model known as the nursing process (Bickford, Marion, & Gazaway, 2015).
National Patient Safety Goals
The National Patient Safety Goals (NPSGs) were established in 2002. The purpose of the NPSGs was to address concerns about patient safety raised by a report from the Institute of Medicine (IOM). The IOM is a Quality Health Care in America committee, which is a division of the National Academies of Science, Engineering, and Medicine.
To Err Is Human
The report, To Err is Human: Building a Safer Health System (Institute of Medicine [IOM], 1999) was a result of two major research studies that found that approximately 98,000 people died each year from medical errors (see Table 5.1). The IOM discovered that these patient deaths were not a result of individual errors, but from a decentralized and fragmented health care system. Among the problems that commonly occur during the course of providing health care are adverse drug events and improper transfusions, surgical injuries and wrong-site surgery, suicides, restraint-related injuries or death, falls, burns, pressure ulcers, and mistaken patient identities (IOM, 1999, p. 1). The IOM also found that many of these errors occurred in areas such as operating rooms, intensive care units, and emergency rooms (IOM, 1999).
Table 5.1
Types of Errors
Diagnostic
Treatment
Preventive
Other
- Error or delay in diagnosis
- Failure to employ indicated tests
- Use of outmoded tests or therapy
- Failure to act on results of monitoring or testing
- Error in the performance of an operation, procedure, or test
- Error in administering the treatment
- Error in the dose or method of using a drug
- Avoidable delay in treatment or in responding to an abnormal test
- Inappropriate (not indicated) care
- Failure to provide prophylactic treatment
- Inadequate monitoring or follow-up of treatment
- Failure of communication
- Equipment failure
- Other system failure
Note. Adapted from To Err Is Human: Building a Safer Health System Report Brief, by the Institute of Medicine, 1999, p. 2. Copyright 1999 by the Institute of Medicine.
The IOM committee developed four recommendations to lead the way to making healthcare safer. The first recommendation called for the creation of a National Center for Patient Safety within the U.S. Department of Health and Human Services (HHS) Agency for Healthcare Research and Quality (AHRQ). This designated organization would be responsible for establishing NSPGs and tracking their progress. The second recommendation was to create a mandatory reporting system to collect data regarding medical errors. This provided the IOM with a way to track errors and information to prevent future errors and harm. The third recommendation called upon patients, healthcare professionals, and accreditation groups to put pressure on healthcare organizations to provide a safer environment for patients. The only way to find errors within a system is to report errors and then investigate how and why the error occurred.
An error causing an adverse event could have been a patient safety event or an error in documentation. No matter the reason for the adverse event, stopping its cause is paramount. The IOM (1999) report focused on errors that occurred in health care organizations that lead to patient deaths. Analysis of reported errors has revealed many hidden dangers, such as near misses, dangerous situations, and deviations or variations that point to system vulnerabilities, not intentional acts of clinician performance that may eventually cause patients harm (Wolf, 2008). Part of providing quality care is to be aware of events that could occur and could cause harm.
Pressure was applied in the creation of quality indicators, which are measurements of the delivery of quality care. For example, it has been decided the development of hospital-acquired pressure ulcers is a direct indicator of poor care delivery. A patient receiving quality care should never develop a pressure ulcer. So, each month, every organization must report whether any patients developed a pressure ulcer. If so, the organization might not receive the monetary incentive for quality care delivery provided by HHS and Centers for Medicare & Medicaid Services (CMS). Organizations able to prove that zero patients acquired pressure ulcers would receive the monetary incentive.
The last recommendation was to build a culture of safety. Creating and sustaining a culture of safety would require actions by thousands of health care organizations. Hospital leadership must provide resources and time to improve safety. The organizational culture must encourage recognition and learning from errors (Donaldson, 2008, p. 5). It is important for all RNs to participate in building and maintaining a culture of safety while working. Those in leadership positions must lead by example in maintaining a culture of safety.
Health care organizations must change and adopt new ways of providing patient care while maintaining a culture of safety. New ways of providing safe care have been developed and are still being developed by conducting studies and finding new and innovative ways for RNs to provide safe, quality care. Hospitals must report errors and explore why errors occurred and what they can do to prevent errors from reoccurring. Safety is now a hospitals priority.
The Joint Commission
In 2002, The Joint Commission (TJC) established the NPSGs. Health care organizations now have indicators, which are measured to assure a culture of safety. The group that developed the NPSGs was composed of nurses, physicians, and other health care professionals who had first-hand knowledge and experience regarding patient safety. They identified a wide variety of patient safety issues. This group is known as the Patient Safety Advisory Group. They work closely with TJC to continue identifying ongoing issues (The Joint Commission [TJC], 2017).
When issues are found by TJC, the organization must develop action plans to correct any deficiencies that were found and report back to TJC regarding any changes that were implemented. Many times, committees composed of multidisciplinary health care professionals are formed to find solutions for the problems associated with the deficiencies. These deficiencies become the foundation for new safety procedures and regulations that were adopted to correct TJCs findings.
Crossing the Quality Chasm
In 2001, the IOM published Crossing the Quality Chasm: A New Health System for the 21st Century, which has shaped the future of health care. Again, the IOMs report found that many patients died in the hospital while receiving care. The IOM believed there was not only a gap in health care that contributed to unnecessary patient deaths but a chasm. Contributing to the problems faced by a rapidly changing system because of advancements in technology and medicine, people were living longer. Living longer leads to an increase in chronic conditions such as heart disease, respiratory illnesses, and diabetes (IOM, 2001). Crossing the Quality Chasm: A New Health System for the 21st Century focuses on how the health system can be re-invented to foster innovation and improve the delivery of care (IOM, 2001, p. 2). The report discussed six goals for improvement, which included safety, providing effective medical care, providing patient-centered care in a timely, efficient, and equitable way. The hope was for patients to receive care that was delivered in a safe and reliable environment producing healthier, satisfied patients. As a result, Congress established the Health Care Quality Innovation Fund. The committee listed 10 general rules to follow while redesigning the health care system to achieve safer, patient-centered care (see Table 5.2). Most of what is expected from the BSN-prepared nurse focuses on providing safer, quality care. Knowing the 10 general rules prepares the nurse for the expectation of care.
Table 5.2
Ten Rules for Redesign
Rule
Explanation
- Care is based on continuous healing relationships.
Patients should receive care whenever they need it and in many forms, not just face-to-face visits. This implies that the health care system must be responsive at all times, and access to care should be provided over the Internet, by telephone, and by other means in addition to in-person visits.
- Care is customized according to patient needs and values.
The system should be designed to meet the most common types of needs but should have the capability to respond to individual patient choices and preferences.
- The patient is the source of control.
Patients should be given the necessary information and opportunity to exercise the degree of control they choose over health care decisions that affect them. The system should be able to accommodate differences in patient preferences and encourage shared decision making.
- Knowledge is shared and information flows freely.
Patients should have unfettered access to their own medical information and to clinical knowledge. Clinicians and patients should communicate effectively and share information.
- Decision making is evidence-based.
Patients should receive care based on the best available scientific knowledge. Care should not vary illogically from clinician to clinician or from place to place.
- Safety is a system property.
Patients should be safe from injury caused by the care system. Reducing risk and ensuring safety require greater attention to systems that help prevent and mitigate errors.
- Transparency is necessary.
The system should make available to patients and their families information that enables them to make informed decisions when selecting a health plan, hospital, or clinical practice, or when choosing among alternative treatments. This should include information describing the systems performance on safety, evidence-based practice, and patient satisfaction.
- Needs are anticipated.
The system should anticipate patient needs, rather than simply react to events.
- Waste is continuously decreased.
The system should not waste resources or patient time.
- Cooperation among clinicians is a priority
Clinicians and institutions should actively collaborate and communicate to ensure an appropriate exchange of information and coordination of care.
Note. Adapted from Crossing the Quality Chasm: A New Health System for the 21st Century Report Brief, by the Institute of Medicine, 2001, p. 3-4. Copyright 1999 by the Institute of Medicine.
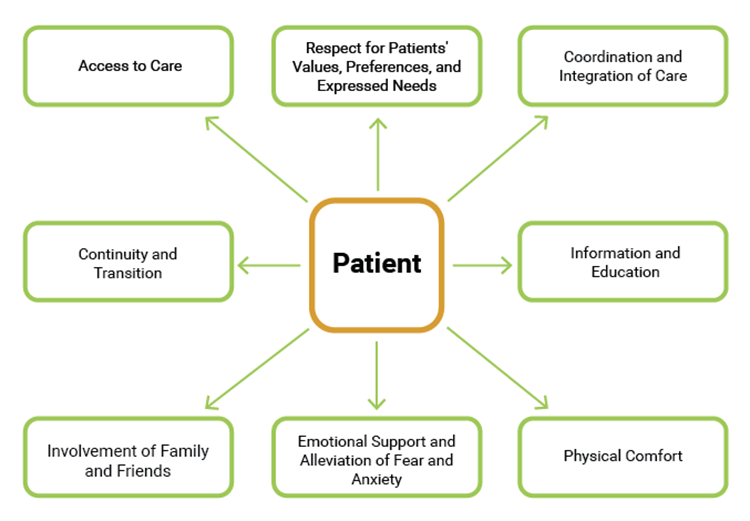
The reports published by the Institute of Medicine (1999; 2001) both focused on building a safer health care system by providing a culture of safety to provide patient-centered care (see Figure 5.1). The IOM defines patient-centered care as Providing care that is respectful of, and responsive to, individual patient preferences, needs and values, and ensuring that patient values guide all clinical decisions (IOM, 2001, p. 3).
Figure 5.1
Patient-Centered Care
 fullscreenClick here to enlarge
fullscreenClick here to enlarge
Note. Adapted from A 2020 Vision of Patient-Centered Primary Care, by K. Davis, S. C. Schoenbaum, and A. Audet, 2005, Journal of General Internal Medicine, 20(10), 953-957. Copyright 2005 by the Journal of General Internal Medicine.
Goals Set in Response to Reports
As a part of the IOM reports, the Joint Commission established the first set of the NSPGs in 2002. Initially, there were six goals for the health care system to implement and 11 recommendations by the Patient Safety Advisory Group. By implementing these very specific changes to the health care system, patient care would be safe, and there would be fewer hospital-related deaths.
Table 5.3
National Safety Patient Goals Implemented in 2003
Goal 1
Improve the accuracy of patient identification.
Goal 2
Improve the effectiveness of communication among caregivers.
Goal 3
Improve the safety of using high-alert medications.
Goal 4
Eliminate wrong-site and wrong patient procedure surgery.
Goal 5
Improve the safety of using infusion pumps.
Goal 6
Improve the effectiveness of clinical alarm systems.
Note. Adapted from Special Edition: JCAHO Patient Safety Goals 2003, by the National Center for Patient Safety, 2002, Topics in Patient Safety (TIPS), 2(5), p. 2-10. Copyright 2002 by the National Center for Patient Safety.
Many NSPGs are well known by RNs because the goals have become a part of everyday practice. To have no hospital-acquired pressure ulcers, central-line infections, and catheter-associated urinary tract infections are three of the goals for hospitals to achieve. As BSN-prepared nurses, it is important to be knowledgeable and lead other RNs to practice and comply with the standards set forth for patient safety and professional practice. Providing a patient-centered health care experience for the patient is what health care is all about. Having baccalaureate-prepared RNs who are educated regarding the NPSGs will help ensure a culture of safety.
Many of the NPSGs have not changed significantly from what they were in 2003. The goals continue to change and evolve toward providing a culture of safety as new evidence is brought forward. There was another national campaign at the time that focused on providing quality care and ensuring a safe patient environment. The 100,000 Lives Campaign was introduced by the Institute for Healthcare Improvement (IHI). This campaigns goal was to decrease morbidity and mortality caused by medical errors nationally.
The IOM has continued to focus on improving health care and the health care system. With each new report comes new and innovative ways to build a safer system. In 2010, the IOM and the Robert Wood Johnson Foundation published The Future of Nursing: Leading Change, Advancing Health, which contained four recommendations to advance the practice of nursing:
- Nurses should practice to the full extent of their education and training.
- Nurses should achieve higher levels of education and training through an improved education system that promotes seamless academic progression.
- Nurses should be full partners, with physicians and other health care professionals, in redesigning health care in the United States.
- Effective workforce planning and policy making require better data collection and information infrastructure (National Academies of Science Engineering Medicine, 2015, para. 2).
The importance of these four recommendations affect every nurse. Nurses will now be expected to practice to the full extent of their education and training. Nurse practitioners will be major providers of health care. Becoming a BSN-prepared nurse fulfills the second recommendation of achieving higher levels of education and engaging in lifelong learning. Nurses are now working as members of the health care team in a multidisciplinary environment by partnering with physicians and other health care professionals.
Structured Communication Tools
Structured communication is using a consistent format when providing information. Effective communication was one of the areas the IOM established as an area in need of improvement so hospitals could provide a culture of safety in which patients could receive safe care. In 2008, TJC identified effective communication as one of its NSPGs (Dunsford, 2009). Communication failures were found to result in loss of life. This goal targeted communication not only between physician and patient, but also between patient and all other health care professionals.
ISBAR
In 2002, a group of clinicians revised a tool used by the U.S. Navy for standardizing urgent communication in nuclear submarines (Marshall, Harrison, & Flanagan, 2008) into an effective communication tool for health professionals, which is now known as SBAR communication.
- Situation: Opening statement to describe the current situation
- Background: History about the current situation
- Assessment: Information found upon assessment
- Recommendation: What the person is requesting to be done
The IHI, established in 1991 to focus on quality improvement in health care, promotes using SBAR for patient safety. The IHI (Institute for Healthcare Improvement [IHI], n.d.a) states the SBAR method of communication allows for an easy and focused way to set expectations for what will be communicated and how it will be communicated between members of the team, which is essential for developing teamwork and fostering a culture of patient safety (para. 3). Structured communication is an efficient and accurate method for interdisciplinary communication, which promotes a culture of safety.
SBAR communication is now a widely accepted form of communication when nurses are communicating information to physicians, such as a change in the patients condition or reporting newly acquired laboratory values or test results. The letter I, standing for identification, is a recent addition to the SBAR tool. When employing ISBAR communication, nurses should identify themselves before any information is shared, so information is not given to the wrong person. BSN-prepared nurses are responsible for ensuring proper communication occurs between the physician and other members of the health care team.
Table 5.4
ISBAR
Definition
Example
Identification
To provide your name to the receiver of information
Good morning, Dr. Pasquale. This is Gina calling with information regarding Mr. Enrico.
Situation
Opening statement to describe the current situation
Mr. Enrico is requesting pain medication for his back pain.
Background
History about the current situation
Mr. Enrico is a 62-year-old male who was involved in a motor vehicle accident three hours ago.
Assessment
Information found upon assessment
Mr. Enrico is complaining of severe back pain from his lower back down his left leg. B/P is 170/90, heart rate 112, and respirations are 24. He is afebrile. He has no visible injuries to his back.
Recommendation
What the person is requesting to be done
I am requesting pain medication for my patient Mr. Enrico.
Note. Adapted from SBAR Tool: Situation-Background-Assessment-Recommendation, by the IHI, n.d. Copyright n.d. by the IHI.
Universal Protocol
Another form of structured communication is the Universal Protocol for preventing surgery from being performed on the incorrect patient or on the incorrect site. It also prevents incorrect procedures from being performed on patients. According to the AHRQ (Agency for Healthcare Research and Quality [AHRQ], n.d.), wrong-site surgery occurred at a rate of approximately 1 per 113,000 operations between 1985 and 2004. In July 2004, The Joint Commission enacted a Universal Protocol that was developed for preventing wrong-site, wrong-procedure, and wrong-person surgery (para. 1).
Protecting surgical patients is one of the NSPGs and is called time-out. Time-out was developed to protect the patient from harm when undergoing any procedure. The Universal Protocol starts with a preprocedure checklist to verify the correct patient, the correct procedure, and the correct site. If possible, the patient should be included in this process. The patient, along with the provider, will mark the site where surgery is being done with a marker to assure that the surgery is performed on the correct side. The time-out includes all members of the procedure team, including the physician, nurse, anesthesiologist, and any other active participants in the procedure. When the time-out begins, all members of the team must immediately stop what they are doing and pay attention to the team member who is completing the time-out duties. During the time-out, the team must all agree they have the correct patient, the correct site marked for surgery, and the right procedure to be performed on the patient. The institution where the surgery is being performed may include more verifications. At the end of the time-out, proper documentation must also be completed in the electronic health record (TJC, n.d.). Many times, it is the BSN-prepared nurse who will start the time-out process for the team.
Integrated Health Care Priorities
Patient safety and patient-centered care are two priorities of Americas health care system. One focus of patient care is for health professionals to start providing care in the community by educating the public about prevention of disease and illness. By providing education to the patient, the BSN-prepared nurse may prevent hospital readmissions and keep the patient healthy and at home. Health and wellness have become the priority of many health care providers. The National Center for Complementary and Integrative Health (NCCIH) is the Federal Governments lead agency for scientific research on the diverse medical and health care systems, practices, and products that are not generally considered part of conventional medicine (National Center for Complementary and Integrative Health [NCCIH], 2017, para. 1). The NCCIH hopes to find new and innovative ways to provide health care by combining conventional medicine with alternative nonpharmacologic therapies. The NCCIH is conducting research to discover alternative therapies that will promote wellness and prevention (see Table 5.5). Nonpharmacologic therapies are important for the professional nurse to know so alternatives to pain medications can be suggested. The opioid problem in the United States contributes to the need for nonpharmacological alternatives.
Table 5.5
Most Common Nonpharmacologic Therapies
Example
Example
Natural Products
Most Common
Deep Breathing
Yoga, Tai Chi, or Qi Gong
Chiropractic or Osteopathic Manipulation
Meditation
Massage
Special Diets
Homeopathy
Progressive Relaxation
Guided Imagery
Least Common
Note. Adapted from Complementary, Alternative, or Integrative Health: Whats in a Name? by the National Center for Complementary Care and Integrative Health, 2017b, paras. 12-13, Copyright 2017 by the National Center for Complementary Care and Integrative Health.
Quality and Safety Education for Nurses (QSEN)
The Quality and Safety Education for Nurses (QSEN) project was started in 2005 and is funded by the Robert Wood Johnson Foundation. The Quality and Safety Education for Nurses (QSEN) project addresses the challenge of preparing future nurses with the knowledge, skills, and attitudes (KSA) necessary to continuously improve the quality and safety of the health care systems within which they work (QSEN Institute, 2017, para. 1). QSEN has been able to provide educators with information about the numerous quality competencies necessary for nurses to possess in a prelicensure program, as well as RNs who are furthering their education to become baccalaureate-prepared nurses and advanced practice nurses. QSEN also works on providing the KSAs for nurses to provide safe, competent care by educating nurse educators to provide these skills to nursing students. QSEN supports nursing to work within a multidisciplinary environment and to include ancillary services such as social work and case management to be active participants in ensuring patient-centered care. QSEN is also involved in the knowledge, skills, and attitudes for the advanced practice nurse and in strategies to promote curric